What is Mohs Micrographic Surgery?
Mohs Micrographic Surgery has the highest cure rate as well as the lowest rate of recurrence. Of the many and varied options of cancer treatments available today, Mohs Micrographic Surgery results in the smallest possible defect allowing for the optimum cosmetic result.

The Surgery
Mohs Micrographic Surgery (MMS) is the technique used in the removal of Basal Cell Carcinomas and Squamous Cell Carcinomas.
MMS is the most advanced and effective of the techniques available today, for the removal of these two most common forms of skin cancer.
Mohs Micrographic Surgery has a successful cure rate of 99%.
This rate is well above all other current cancer treatment success rates available today.
The Origins
 Originally developed in the 1930’s by Dr. Frederic Mohs, the Mohs Micrographic Surgery technique has evolved over many years to having the highest cure rate, and is now practiced successfully, worldwide.
Originally developed in the 1930’s by Dr. Frederic Mohs, the Mohs Micrographic Surgery technique has evolved over many years to having the highest cure rate, and is now practiced successfully, worldwide.
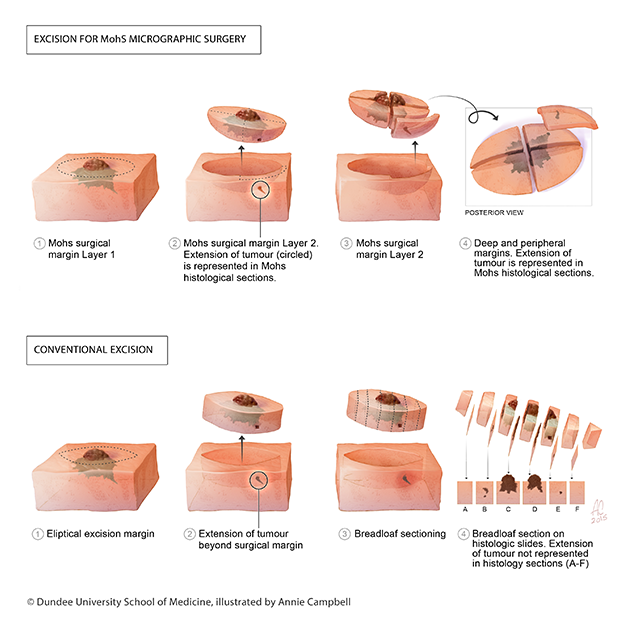
The point of difference for MMS is in the immediate microscopic examination of the tissue surrounding the excised area, including examination of 100% of the border to ensure that all extensions of the tumour have been removed completely.
In conventional surgery only around 1% of the tissue margin is examined which means that some ‘roots’ may go unnoticed until the tumour re-occurs.
During Mohs surgery, repeated stages are taken followed by microscopic examination, until the Mohs Surgeon is able to ascertain with certainty that the tumour or lesion has been completely removed. Because the doctor can see immediately what needs to be removed, very little uninvolved healthy tissue is excised.
Most patients require one or two stages to achieve clearance.
The Benefits
✔️Highest chance of removing every cell of tumour on the first day of surgery.
✔️Lowest chance of the tumour ever growing back.
✔️The most effective way to reduce loss of surrounding healthy tissue.
✔️Because less healthy tissue is lost, the wound repair will give the best functional and cosmetic outcomes.
✔️We use local anaesthetic which is much safer than general anaesthetic.
MMS has been used in practice since the 1930’s and there is an abundance of good quality studies providing the medical evidence of its effectiveness. An example of this is a large study looking at new or recurrent basal cell carcinoma on the face. They found that after 5 years:
Those tumours removed with conventional surgery 12.1% of tumours re-occurred. Those removed with Mohs Surgery. Only 2.4% of tumours re-occurred.
Source: Lancet Oncol. 2008 Dec;9(12):1149-56. doi: 10.1016/S1470-2045(08)70260-2. Epub 2008 Nov 17. Surgical excision versus Mohs' micrographic surgery for primary and recurrent basal-cell carcinoma of the face: a prospective randomised controlled trial with 5-years follow-up. Mosterd K1, Krekels GA, Nieman FH, Ostertag JU, Essers BA, Dirksen CD, Steijlen PM, Vermeulen A, Neumann H, Kelleners-Smeets NW.
Steps Involved
Mohs Micrographic Surgery (MMS) is performed as a single day procedure under local anaesthesia. MMS involves the following steps:
01 Defining an Area for Removal
The visible area of the lesion or tumour is outlined on the skin using a specialist marker. This area includes a small margin. A reference map or grid is also drawn on the patient. Sometimes the use of temporary sutures is most effective in this step.
02 Removal of Target Area
The area, as marked and described above, is surgically removed with an angle of thirty to forty-five degrees at the radial margins.
03 Temporary Dressing of the Area
Haemostasis (stopping of the flow of blood) is obtained, this is followed by the wound being temporarily dressed.
04 Division of Removed Sample
The sample of tissue that has been excised (surgically removed) is then divided into two or more sections. These sections are colour-coded using special tissue dyes, developed for this purpose.
05 Tissue Mapping
This step is the tissue mapping process, which ensures later matching between the residual tumour examined under microscope, and its exact original location on the patient. We use a paper-based map or digital photographs as well as image processing software
06 Freezing of the Sample
This step is performed by a specialised biomedical scientist, who embeds and freezes the removed tissue into a cryostat (an apparatus for maintaining very low temperature) for the purpose of creating horizontal sections of the entire excision
07 Sample Examined
The sample sections are microscopically examined by the Mohs Surgeon, who determines if there is any remaining cancer.
08 Tissue Mapping Updated
The Mohs Surgeon updates the tissue map by precisely drawing on the map or digital image.
09 Tissue Map Referral
The area on the patient where further tissue needs to be removed is determined by identifying the area on the map.
10 Excision Process Repeated
The process of tissue removal is repeated from Step 2, until the tumour or lesion is no longer present in the patient’s tissue.
11 Wound Closure
At this final stage, the wound is closed. There are a variety of available techniques that the Mohs Surgeon can perform to achieve optimum results, and the technique will be at their discretion based on the wound size, location, and other factors.